Management of Multiple Trauma Patient
Early Total Care
Solayar GN
Sydney Knee Specialists, St. George’s Hospital, Sydney, Australia
Surgical intervention in the multiple trauma patient is controversial. One is faced with the dilemma of early fixation to promote accelerated rehab and avoid the consequences of prolonged immobility versus the potential hazards of the secondary hit when performing operations on an already physiologically compromised patient.
The concept of waiting for physiologic stabilisation prior to performing long bone fixations stems from research on multiple trauma patients in the 1960s. Immediate fixation via intramedullary nailing was associated with unacceptably high morbidity and mortality rates from fat embolisms, pulmonary embolisms and poor cardio-respiratory support [7].
Without early fixation, the patient is forced to undergo a period of immobilisation which in itself is fraught with complications. These risks include pneumonia, decubitus ulcerations, vascular coagulopathies, gastrointestinal stasis (increasing the likelihood of aspiration) and psychological detriments. It is associated with longer intensive care stay, hospitalisation and leucocytosis. On the musculoskeletal front, immobility is associated with joint stiffness which may result in permanent arthrofibrosis and disuse muscular atrophy which could limit or delay rehabilitation post injury [2].
In the 1980s, there was a shift towards early total care to minimise the risks of delayed surgery. The development of pulmonary complications (acute respiratory distress syndrome (ARDS), fat embolism and pneumonia) in the multiply injured patients were reduced via early fixation compared to delayed stabilisation. The patient is rehabilitated earlier thus avoiding the risks of prolonged immobilisation as mentioned previously. There were also improved outcomes in terms of hospitalisation period and overall costs [1]. Limitations on this included the loose definition of 'early care' as it included fixation timings of under 6 hours up to 3-4 days.
Appropriate fixation timing must respect the individual nature of the overall physiology and condition of each poly-traumatised patient. The immune system is subjected to an early hyper-inflammatory phase which may be followed by a hypo-inflammatory period which often precedes multiple organ failure. Aggressive and prolonged surgery may tip this delicate inflammatory balance and compromise potential gains with detrimental effects to surgical subject [3].
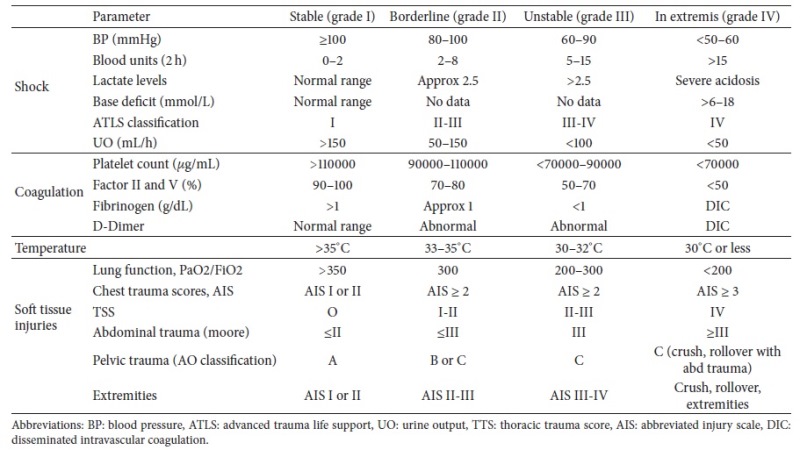
The key for management involves expedient and efficient resuscitation immediately following injury. Managing blood loss, coagulopathy and temperature is paramount at the initial stage. There are several parameters which may be used to identify patients which would be suitable for early stabilisation. By employing the Injury Severity Score (ISS) and Abbreviated Injury Score (AIS), it is suggested that patients be divided into 4 groups (stable, borderline, unstable and in extremis). Early total care is considered for those patients in the former 2 categories and it is recommended that surgical time be kept under 2 hours [6]. These categories are summarised in Table 1 by Nicola R (2013) Early Total Care versus Damage Control: Current Concepts in the Orthopedic Care of Polytrauma Patients. ISRN Orthop. 2013:329452 [5]:
Specific systems such as head injuries and chest injuries were historically thought to be relative contraindications towards early surgery. These concepts have been challenged in recent literature and the debate continues. Nahm et al found that patients with Severe (Abbreviated Injury Scale score ≥3) abdominal injury was associated with more complications than severe head (Glasgow Coma Scale score ≤8) and chest (Abbreviated Injury Scale score ≥3) injuries in patients with early definitive fixation [4]. Studies by Weninger et al, and Brundage et al, also indicate that early fixation does not increase pulmonary complications following chest injuries when compared to delayed stabilisation [2,8].
In summary, early total care should be considered in stable and borderline patients. With more advancements regarding early resuscitation, patient selection and medical management, the outcomes following early total care is forecasted to improve; negating the detrimental effects of prolonged immobilisation and longer hospitalisation. Patient selection remains the key consideration when choosing between early total care and damage control orthopaedics.
References:
- Bone LB, Johnson KD, Weigelt J, Scheinberg R (1989) Early versus delayed stabilization of femoral fractures. A prospective randomized study. J. Bone Joint Surg. Am. 71:336–40
- Brundage SI, McGhan R, Jurkovich GJ, Mack CD, Maier R V (2002) Timing of femur fracture fixation: effect on outcome in patients with thoracic and head injuries. J. Trauma 52:299–307
- Giannoudis P V, Abbott C, Stone M, Bellamy MC, Smith RM (1998) Fatal systemic inflammatory response syndrome following early bilateral femoral nailing. Intensive Care Med. 24:641–2
- Nahm NJ, Como JJ, Wilber JH et al. (2011) Early appropriate care: definitive stabilization of femoral fractures within 24 hours of injury is safe in most patients with multiple injuries. J Trauma. Jul;71(1):175-85
- Nicola R (2013) Early Total Care versus Damage Control: Current Concepts in the Orthopedic Care of Polytrauma Patients. ISRN Orthop. 2013:329452
- Pape H-C, Giannoudis P V, Krettek C, Trentz O (2005) Timing of fixation of major fractures in blunt polytrauma: role of conventional indicators in clinical decision making. J. Orthop. Trauma 19:551–62
- Smith JE (1964) The results of early and delayed internal fixation of fractures of the shaft of the femur. J. Bone Joint Surg. Br. 46:28–31
- Weninger P, Figl M, Spitaler R, Mauritz W, Hertz H (2007) Early unreamed intramedullary nailing of femoral fractures is safe in patients with severe thoracic trauma. J. Trauma 62:692–6
Damage Control Orthopaedics
Syah Bahari
KPJ Seremban Specialist Hospital & KPJ Healthcare University College, Malaysia
There has been a decades long debate between early total care (ETC) and damage control orthopaedics (DCO). Early total care was popularised in the 70s and 80s where success of early fixation of femoral fractures was shown to have better outcome and less pulmonary complications. The arguments for early fixation of femoral fracture is to minimise hemorrhage from fracture site, prevent ongoing soft tissue damage and minimise systemic inflammatory activation thus reducing secondary lung complications. A landmark paper by Bone et al (1989) [1] showed in a prospective clinical trial that patients underwent definitive femoral fracture stabilisation within 24 hours of admission and showed significant reduction in lung complications when compared to patients which were delayed.
However, in a subgroup of the severely injured patients, early definitive fixation of fractures may not be appropriate. A study by Pape et al (2002) [2] showed that, in the multiple trauma patients specifically if they sustained chest injuries, early total care resulted in significantly more pulmonary complications. The argument for damage control orthopaedics is to minimise the 'second' hit to the systemic inflammatory system, which was due to surgical trauma caused by the surgical stabilisation of fractures. The authors subsequently categorises the multiple injured patients into 4 groups, which are stable, borderline, unstable, and extremis based on their level of injuries and physiological response at time of presentation.
More recent studies published debating these 2 concepts of management of multiple trauma patients supports that ETC is appropriate in the stable and borderline multiple injured patients and DCO is the best option for management of patients which are unstable and in the extremis [3,4].
Therefore, the current debate should not be which management is better but which patients would be better treated with either ETC or DCO.
To quantify the severity of the injury, the Injury Severity Scale (ISS) has been used extensively in clinical trials, research and also clinical pathway in patient transfer to a major trauma centre but not specific for decision-making for definitive treatment [5]. Measuring the systemic response using Interleukin 6 (IL-6) has been shown to be specific in determining the severity of injury [6] but this modality is not available in most trauma centres.
A practical approach is to quantify the physiological response to resuscitation in the multiple trauma patients. End organ hypo perfusion has been associated with these patients [7]. Vallier et al (2013) [8] coined the term early appropriate care, where in their study of 1,442 patients with pelvic, spinal and/or femoral fractures, the patients underwent comprehensive resuscitation prior to definitive surgical fixation. In their paper, patients with lactate level < 4.0mmol/L, pH > 7.25 or base excess > 5.5mmol/L post resuscitation were safe to proceed with definitive fixation. However, patients which were not responsive to resuscitation, where the lactate, pH and base excess were worsening, were treated with DCO. DCO is reserved for patients who are not responsive to resuscitation within 8 hours and definitive treatment can commence when the parameters above normalise.
In conclusion, both ETC and DCO have their place in the management of multiple trauma patients. Comprehensive resuscitation is key to improve end organs hypo perfusion. Future research should be focused on improving resuscitation protocol and finding more practical methods to measure the physiological response to resuscitation.
References:
- Bone LB, Johnson KD, Weigelt J et al. (1989) Early versus delayed stabilisation of femoral fractures. A prospective randomized study. J Bone Joint Surg Am. 71:336-340
- Pape HC, Hildebrand F, Pertschy S et al (2002) Changes in the management of femoral shaft fractures in polytrauma patients: from early total care to damage control orthopedic surgery. J Trauma. 53:452-461
- Nicholas B, Toth L, van Wessem K et al. (2011) Borderline femur fracture patients: early trauma care or damage control orthopaedics? ANZ J Surg. 81:148-153
- Morshed S, Corrales LA, Lin K et al. (2011) Femoral nailing during serum bicarbonate-defined hypoperfusion predicts pulmonary organ dysfunction in multisystem trauma patients. Injury. 42:643-649
- Senkowski CK, McKenney MG (1999) Trauma scoring system: A review. J AM Coll Surg. 189(5): 491-503
- Roberts CS, Pape HC, Jones AL et al. (2005) Damage control orthopaedics: evolving concepts in the treatment of patients who have sustained orthopaedic trauma. Instr Course Lect. 54:447-462
- Blow O, Magliore L, Claridge JA et al. (1999) The golden hour and the silver day: detection and correction of occult hypoperfusion within 24 hours improves outcome from major trauma. J Trauma. 47:964-969
- Vallier HA, Wang X, Moore TA et al. (2013) Timing of orthopaedic surgery in multiple trauma patients: development of a protocol for early appropriate care. J Orthop Trauma. 27:543-551










